Facial Cancer Reconstruction
Cancer treatment in the face may leave large facial wound or wound in critical area of the face (such as the eyelid, the mouth, or the nose) that requires complex reconstruction including microsurgery.
The most common cancer in the head and neck areas are skin cancers. These include basal cell carcinoma, squamous cell carcinoma, and melanoma. Resection of these skin cancer with possible lymph node biopsy are the main treatment for cancers that can be removed safely. If the cancer cannot be removed completely, radiation may be indicated. Reconstruction is generally delayed until there is confirmation that all cancerous tissue is removed. In case of Moh’s excision (excision combined with on-site tissue evaluation of cancer), reconstruction can be performed immediately or shortly after the excision.
Other type of cancers in the head and neck areas are salivary glands, nasal/ oral/ sinuses/ pharynx/ larynx squamous cell carcinoma. Most intranasal/oral/sinuses/pharynx/larynx cancers are treated initially with radiation as resection may leave patients with significant deformity and disability. In small percentage of patients, radiation is not sufficient or there is recurrence of cancer, then resection is indicated. In these cases, reconstruction with free tissue transfer (moving tissue from elsewhere in the body) to reconstruct the defect and restore function may be necessary.
Who is a good candidate for facial cancer reconstruction?
The best candidates are healthy people with realistic expectations of surgery. Patients with medical problems are also candidates for surgery as long as they are in their optimal health and are well informed of their peri-operative risks.
How is the surgery performed?
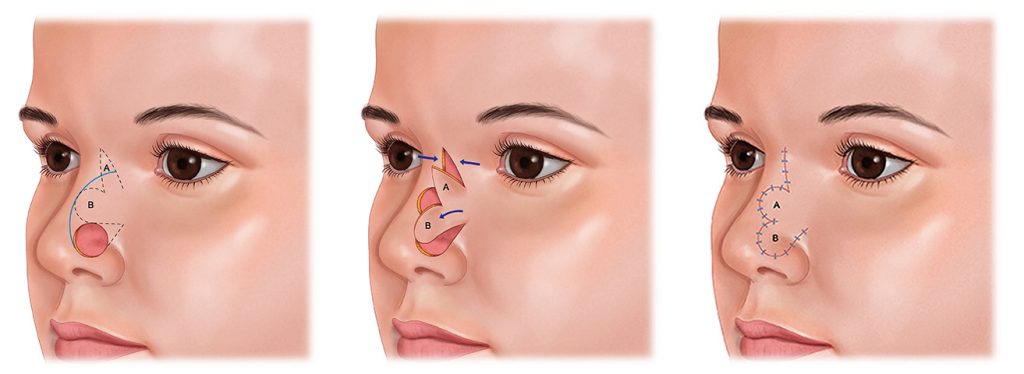
The surgeries vary from simple closure of the wound to microsurgical free flap from a remote site for closure. Some reconstructions require multiple stages. Patients are provided with all reconstructive options and the surgery will be tailored to their specific cancer defect and health status.
What is the recovery?
Downtime from a facial cancer reconstruction is generally 1-2 weeks. Swelling and bruising are expected and should resolved in 1-2 weeks. Depending on the complexity of the reconstruction, patients may stay in the hospital for closed-monitoring for a few days. If staged reconstruction is indicated, timing between surgeries is generally 3-4 weeks.