Facial Feminization
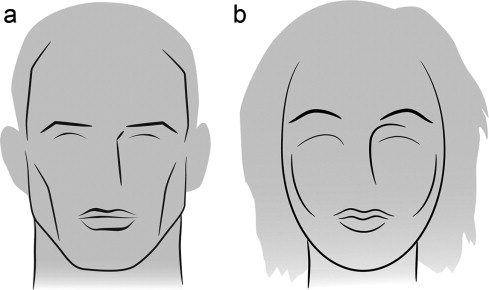
Facial feminization surgeries (FFS) involve a set of procedures which aim to change typical masculine features to more feminine features. In the face, testosterone exposure often results in frontal bossing, lower eyebrows (sitting at the level of the orbital rim), prominent frontal nasal angle (transition between the forehead and the nose), larger nose, flatter wider cheek, and wide and square jaw. These features are addressed in FFS.
Who is a good candidate?
The best candidates are healthy people with realistic expectations of surgery. World Professional Association for Transgender Health (WPATH) provides standard criteria to guide health professionals to optimize patients medically prior to surgery. This requires pre-operative evaluation and counseling of a psychologist or psychiatrist and a primary care physician. In addition, CT scan of the face is often necessary for surgical planning.
How are the surgeries performed?
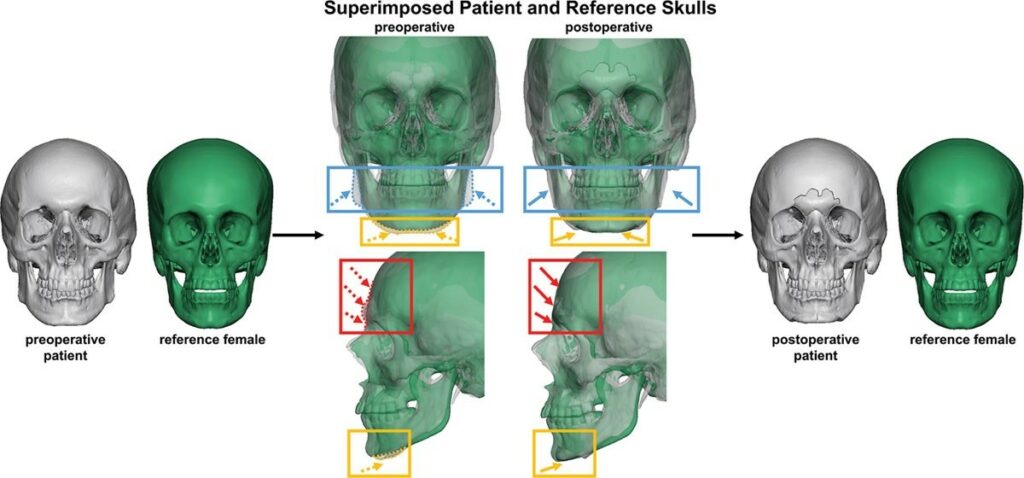
All the steps of the surgery are planned virtually. CT Images of the patient skull is superimposed on a female reference skull to guide the proportional reduction. Most often, forehead reduction, orbital rim reduction, and mandible reduction are required along with feminizing rhinoplasty and fat transfer. The skeletal reduction procedures are performed with pre-cut template from the virtual planning. This minimizes guesswork for the skeletal modification and therefore providing more consistent results.
What is the recovery?
Significant swelling and some bruising can be expected after the surgery. Depending on the number of procedures performed, patients may require overnight stay in the hospital. Downtime from the surgery is approximately 1-2 weeks. Pain and discomfort are normal and can be controlled with pain relief medicine. Some sutures will need to be removed at 1 week after surgery.
Forehead and hairline reduction is almost always recommended as part of facial feminization. Dr. Outerhoust, who is a pioneer in facial feminization surgery, classified the forehead shape and coutour into 4 distinct groups.
- Type I forehead has a minimal or absent frontal sinus, therefore contouring can be achieved with shaving of the bone alone.
- Type II forehead has a protruding anterior wall of the frontal sinus but normal frontal nasal angle (transition between the forehead and the nose). To improve the contour, augmentations of the area above the protrusion can be done with implant or bone cement.
- Type III forehead has over-projected anterior wall of the frontal sinus and acute frontal nasal angle (sharp transition between the forehead and the nose). In this case, forehead reduction requires anterior wall osteotomy (cutting out the front wall of the sinus in the forehead) to allow for setback and reshape the forehead. The frontal nasal angle is also often shaved down.
- Type IV forehead is small and under projected. Forehead contour can be improved with augmentation of the entire forehead with implant or bone cement.
Majority of patients are in type 3 group and virtual surgical planning allows precise and safe reduction.
Hairline reduction is accomplished by releasing the posterior scalp and advancing it forward to shorten the forehead and temporal recess.
Facial femization often requires a combination of procedures. Most commonly necessary procedures are fat transfer, forehead and hairline reduction, and rhinoplasty. Jawline and chin reduction are performed frequently however are not always required.